{kind=link}
{kind=link}
{kind=link}
{kind=link}
North Shore Restorative & Implant Dentistry
Dental Implant Success Rate
Factors which can influence implant success
Dear Doctor,
I thought dental implants had a high success rate. A friend of mine had an implant that failed, can you tell me why?

Dear Brian,
Dental implants traditionally have a very high success rate. The majority of studies that have been done indicate long-term success rates well over 95%. However, there are many factors that can compromise the success rates of implants. These can be divided into three categories: general health concerns, local factors and maintenance issues. It is important to consult with your dentist or dental professional prior to having dental implants placed to determine whether you are a good candidate. Most implant failures can be eliminated through proper case selection.
- General health concerns that may impact an implant’s success include such factors as smoking, certain drugs, osteoporosis, history of radiation treatment, or a compromised immune system.
- Local factors that could impact implants include bone quality, bone quantity, and initial stability of the implant at the time of placement. Bite-related concerns depend upon the amount of stress that the patient will be placing on the implants. When evaluating an implant patient, your dentist has to evaluate whether you clench or grind your teeth. This will impact both the potential short and long-term success of implants.
- Finally there are maintenance issues, while implants are wonderful high-technology replacements for teeth, they need routine maintenance. This includes daily cleaning and continued professional management. Without ongoing professional care, implants just like any other technically sophisticated device are susceptible to breakdown.
I believe that one should have confidence that implants are an excellent choice to replace missing teeth, but feel free to consult with your dental professional about your unique case requirements — how many dental implants you need, your medications, your medical history, and local findings such as bone quality and quantity. If you are properly evaluated by a qualified dental professional and determined to be a good candidate, there is no reason why you cannot have extremely high success rates as do most patients.
Implant Dentistry: The Need for Speed?
Implant Dentistry
The Need for Speed“Same Day Dental Implants”, “Teeth in an Hour”, “Teeth in a Moment”, “Teeth Yesterday”; people will tell you anything to get you in the door! Don’t be mislead or confused by claims and advertisements suggesting dental implants only take one day or hour of your time, because they don’t.
Implant dentistry is one of the greatest dental advancements of our time. By surgically placing a titanium post (the implant) into the jaw, patients are able to replace missing teeth. The new titanium post mimics the root of a tooth and once stable, a crown is added for superior dental function. This eliminates the need for bridgework, partial and full dentures or living without missing teeth.
When doctors advertise their dental implant procedures as “Teeth in a DayTM“, “One Hour Implants”, “Same Day Dental Implants”, they are eluding to the immediate or front load implant procedures. These advertisements are confusing because: 1) multiple appointments are always needed for any implant case: 2) they count on the fact that people are probably ignorant with dental terminology. The one day or one hour hook refers to the surgery only and may or may not include a permanent tooth.
With newer technology spearheaded by companies such as Noble Biocare®, patients can amazingly leave the implant surgery with a provisional (temporary) or permanent crown placed. This allows the patient to leave the surgery esthetically confident and comfortable. Unfortunately, to qualify for the immediate load implant procedure a patient must have good bone quality and no history of infection at the implant placement site among other qualifiers. This currently eliminates a fair amount candidates right off the bat.
Although traditional implant procedures can’t offer same day restorations or crowns, they do help a broader spectrum of people wanting a permanent, low-maintenance, esthetic, functional solution to missing teeth. Depending on the person and which arch of the jaw is being worked on, the process can take two to six months, multiple minor surgeries, and can involve some sort of temporary bridgework or removable appliance. While a bit more inconvenient, totally worth it knowing eventually the smile will be superiorly restored.
It’s amazing how far dental technology has come and I’m proud to support this technology that will and is helping millions. I’m just concerned with claims that take semantic liberties to get people in their office. Once in the door and not a candidate for “Teeth Yesterday”, they can offer traditional implant treatment which you can get through a dentist or doctor you already have a relationship with. Why not herald these procedures as “Implants in Less Time”; I guess it’s not as catchy.
Staging in Implant Dentistry
Dear Doctor,
I have read lately that implants can be done in two ways — either in one or two stages. Could you explain what this means as well as the pros and cons of each method?
 |
| An example of a dental implant placed into the bone and covered by the gum tissue. This will require a second surgery to uncover the implant (two stage implant surgery). |
 |
| An example of a dental implant placed into the bone with a healing abutment attached protruding through the gum tissue (one stage implant surgery). |
Dear Diane,
This is a good question with a rather interesting answer. First a few basics — a dental implant is used to replace a tooth root that eventually becomes anchored in the bone. This essential step for making implants successful is called osseo-integration (“osseo” – bone; “integration” – fusion or joining with).
Placement of dental implants is a surgical procedure requiring precision shaping of the bone to create an osteotomy (“osteo” – bony; “otomy” – reshaping). That’s a very fancy word for the creation of a receptacle or plainly speaking a “hole” or “channel.” Precision is essential so that the bone is protected and cooled during preparation taking care to keep it viable and alive.
Implants must be placed in intimate contact with the bone to facilitate the integration process. When carefully treated, the cells will adhere to the implant surfaces, which are usually made of commercially pure and specially treated titanium — that’s the magic!
Dr. Per-Ingvar Brånemark, the researcher who discovered the osseo-integration process, developed a protocol in which the newly placed implants were left submerged beneath the gum tissues, protected from the bacteria in the environment of the mouth, and free from the trauma of the bite.
After a period of six months, a second small surgical procedure was performed (step or stage two), to re-expose the implant into the mouth. A healing abutment was temporarily used until the permanent crown could be fabricated. Then, by means of a special attachment called a permanent abutment, a crown (the tooth part you see above the gum) was then attached to it. This was the genesis of the two-stage procedure.
Since that time other implant “systems” have been developed that provide for placement of the implants in the bone, leaving them protruding through the gum tissue, essentially constituting a “one stage” system, and eliminating the second stage healing time generally requiring a further 6-8 weeks.
What does this mean in actuality?
Most experienced surgical dental specialists who place implants will probably agree that either choice can be successful in the right circumstances. Whether to use a one or two-stage system or approach today depends on which tooth has been lost (a front tooth which will need a cosmetic solution versus a back tooth which does not require replacement for the short term) as well as the quality of the bone (back teeth are subject to more biting force than front teeth). Not all bone is the same; some is very hard in which case it is relatively easy to stabilize an implant at the time of surgical placement.
Achieving primary stability at the time of surgical implant placement is a good predictor of healing and proper integration with the bone, and is more difficult to obtain where the bone is softer such as in the back areas of the mouth. Think of the difference between oak and balsa wood. Any early movement of the implant, even microscopic, can deter this delicate process in the first month.
However, there are variations of the one stage approach. On occasion, it is possible to immediately place a temporary crown on an implant so that a person can leave their dentist’s office with a tooth. This “one stage” application can sometimes be accomplished after the extraction site has healed or immediately after tooth removal.
When a tooth is removed and an implant is placed at the same time, this is referred to as immediate implant placement. Additionally, an immediate crown is fabricated and simultaneously placed by a restorative dentist. Primary stability in this special situation is critical, requiring great surgical precision, care, and experience. Great care must also be taken to ensure that the crown is out of biting contact with its opposing tooth — and no biting on hard or chewy foods is permitted during the healing or integration phase.
For situations in which people with systemic (general body) disease like diabetes, or smokers, in which healing may be compromised, the balance might be tipped toward choosing a two stage implant system in which it may be advantageous to allow “submerged” healing to occur to avoid any outside influences (plaque or biting forces) from compromising healing.
In either case, whether a one or two stage implant system is used, either can result in great long-term success. Other factors that may enter the mix are the particular implant type, the system (there are multiple on the market — each with different characteristics), and most important, clinical experience and know how. That gets one back to the reality that dentistry is often as much art as it is science.
- Call North Shore Restorative & Implant Dentistry Office Phone Number (516) 484-6394 to schedule an appointment.
- Call Our Office.
Link Between Heart and Gum Disease
The human body is a single unit composed of a seemingly infinite number of biologic processes. However, did you know that abnormalities of almost any of its parts can, and do, have profound effects in multiple areas? For example, the body’s inflammatory and immune (resistance) systems, responsible for defense against infection and promotion of healing, are an active participant in many chronic diseases. And chronic or longstanding diseases, in which attempts to heal are frustrated by continual inflammation and infection, include high blood pressure, diabetes and arthritis among others.
This is also true for Cardiovascular Disease CVD (“cardio” – heart; “vascular” – blood vessel) and periodontal (gum) disease. Indeed, both of these diseases appear to be linked by inflammation. The good news is that, based on current research, we know that if we can reduce the inflammation caused by periodontal disease, we have a good chance of reducing the risks for heart attacks and strokes, both of which are common results of CVD.
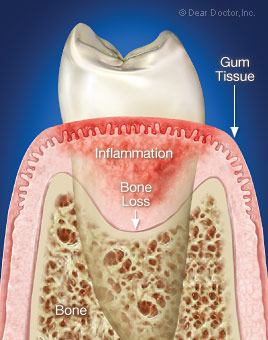
Bodily Effects Of Periodontal Gum Disease
The root causes of periodontal disease are irregular and/or ineffective brushing and flossing. When left, the bacterial biofilms (dental plaque) change over time and lead to the emergence of a small set of highly pathogenic (“patho” – disease; “genic” – causing) organisms that are consistently associated with periodontitis (“peri” – around; “odont” – tooth; “itis” – inflammation). These bacteria both activate and disrupt many of the normal protective mechanisms that help clear them from your mouth. More importantly, if the bacterial biofilm is not removed daily, it activates inflammation in the gums that, in turn, can destroy the connective tissue and bone that support the teeth.
Periodontal disease is a very common disease with mild to moderate forms affecting 30% to 50% of US adults and more severe forms affecting 5% to 15%. It is a silent, painless disease that often occurs without any symptoms. Periodontal disease does produce systemic (bodily) inflammation, but it is not captured by current standard laboratory tests. More sophisticated measures do show markers of inflammation but, in effect, individuals with uncomplicated periodontitis have no signs of infection, such as fever. However, a generalized bodily inflammation smolders in the background like embers of a fire, awaiting the right conditions to be set ablaze. And it is this chronic, low-grade inflammation throughout the body that appears to increase the risk for heart disease and stroke substantially.
Identifying Inflammation Through Routine Blood Tests
Inflammation is not just something that affects your gums, joints and other connective tissues of the body. A study published in the Journal of Periodontology reported that inflammatory effects from periodontal disease cause oral bacterial byproducts to enter the bloodstream and trigger the liver to make proteins such as CRP (C-reactive protein) that inflame arteries and promote blood clot formation that can contribute to clogged arteries leading to heart disease and stroke.
CRP is an inflammatory marker that can be measured by blood tests. A recent study published in The New England Journal of Medicine identified elevated CRP levels as a stronger predictor of heart attacks than elevated cholesterol levels.
In the future, patients could receive routine CRP testing in their dentist’s or periodontist’s office. This could help early identification of risk factors for heart disease or stroke and since patients see their dentist at least twice a year, a significant improvement in early detection may be possible.
Appropriate strategies for treating periodontitis focus on the resolution of inflammation by removing the bacterial biofilm attached to roots of the teeth, along with education to reinforce oral hygiene and reduce bacterial re-growth. Antibiotics may briefly improve sites of localized periodontal infection when combined with professional tooth cleaning to disrupt the biofilm. While antibiotics markedly reduce bacterial amounts, taken alone they do not usually eliminate the disease-causing strains that may be residing in your mouth.
Drugs that modulate or damp down the inflammatory response may reduce the progression of periodontal disease. Low-dose doxycycline, which has an anti-inflammatory effect, is the only FDA-approved drug for treating certain forms of periodontitis. Other non-steroidal anti-inflammatory drugs (e.g., aspirin and ibuprofen) have been extensively studied for use in periodontitis, as have drugs for osteoporosis, such as alendronate, but these are not currently being pursued for periodontal therapy.
Advanced periodontitis may require surgery to gain adequate access to contaminated root surfaces for removal of the bacterial biofilm. In some instances, surgical approaches include bone and soft tissue regeneration to regain at least some support for the teeth and to facilitate bacterial control.
Kindling For The Fire
Environmental and genetic factors, as well as acquired risk factors, are now understood to not only modify, but also accelerate the inflammatory processes in gum disease. Smoking, diabetes, genetics, mental anxiety, depression, obesity, and physical inactivity are strongly linked with increased risk for and severity of periodontitis. Today, approximately 50% of the variation in how severe periodontal disease manifests is explainable by genetic influences.
Periodontal disease is more severe and prevalent in individuals with diabetes, a disorder of the body’s ability to use glucose (normal body sugar) for energy production and its storage, as discussed at length in the Dear Doctor magazine article “Diabetes and Periodontal (Gum) Disease.” Individuals with diabetes and periodontitis also experience a faster rate of loss of tooth-supporting bone than those without diabetes.
Cardiovascular Disease And Inflammation — Bad Connections
Over the past two decades, inflammation has emerged as a factor that is involved in the process of CVD that commonly results in heart attacks and strokes. While the precise role inflammation plays in directly causing chronic CVD remains an area of intense current investigation, much more is now known. And there is both good and bad news regarding the amount and type of fat in the body and its connection to CVD and periodontitis.
 |
| Inflammatory periodontal disease increases inflammation throughout the body. |
First, the bad fat news: Animal fat mainly contains “bad” cholesterol, otherwise known as low-density lipoprotein (LDL), which can cause the accumulation of fat breakdown products within the arterial blood vessel walls. This process leads to an awful sounding condition, atherosclerosis (“athero” – plaque or film; “sclerosis” – hardening and narrowing of arteries). This is also initiated and accelerated by inflammation of the lining of the blood vessels and arteries. So now you can begin to see the potentially terrible connection between your immune system and diseases that have an inflammatory aspect in common. And, unfortunately, your immune system is not always protective.
Inflammation can operate in all stages of CVD, from initiation to progression, and ultimately to complications like heart attacks and strokes, particularly in obese individuals. And the incidence of CVD complications increases in individuals with chronic inflammatory diseases. In addition to periodontitis, they include rheumatoid arthritis, infections of the respiratory (lungs) system, and infections of the urinary (kidney and bladder) tract.
CVD leaves markers in the blood, which can be used to predict complications. For example, higher values of C – Reactive Protein (CRP), a blood marker of inflammation that can predict future heart attacks, unstable angina (chest pain on exertion), the onset of high blood pressure, diabetes, and even stroke.
And Now The Good Fat News
There are current and important strategies that work for preventing CVD, which are centered around reducing dietary fat and lowering LDL (bad) cholesterol with medication. A number of risk factors also relate closely to the development of CVD including age, gender, high blood pressure, diabetes, smoking and low levels of the “good” fat cholesterol, high-density lipoprotein (HDL). With a couple of notable exceptions, most of these factors can be modified by lifestyle changes to reduce risk and improve health. In addition, an individual’s level of chronic inflammation can be monitored by a blood test for CRP and one’s level of inflammation can be reduced by various actions. The most direct approaches to reducing chronic inflammation include reducing body weight, especially around your waist, kicking the smoking habit, getting regular moderate exercise, and controlling untreated inflammatory diseases such as periodontitis.
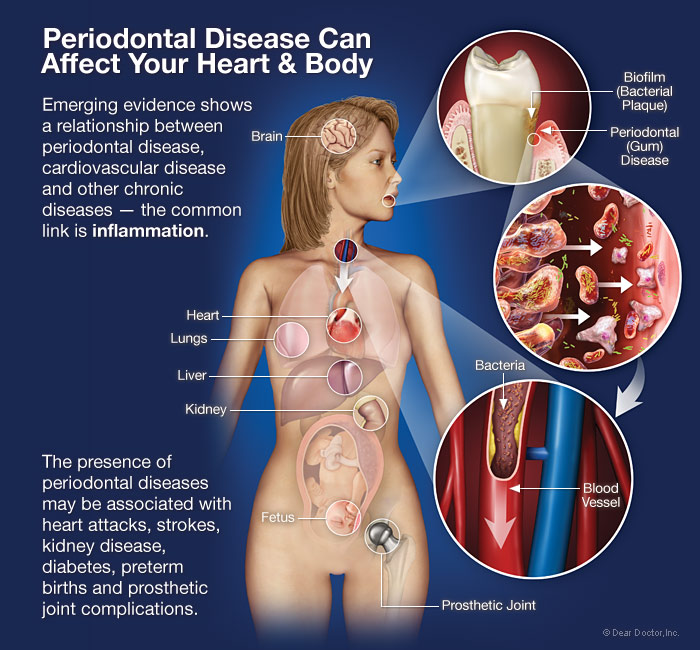 |
| Periodontal Disease Can Affect Your Heart & Body Emerging evidence shows a relationship between periodontal disease, cardiovascular disease and other chronic diseases — the common link is inflammation. Click to enlarge |
Things Just Tend To Add Up
While a direct relationship between periodontitis and CVD has not been established, evidence supports biologically plausible mechanisms. We know that:
- Moderate to severe periodontitis increases the level of systemic (bodily) inflammation – a characteristic of all chronic inflammatory diseases. Sufficient treatment of periodontitis to reduce clinical signs of the disease also decreases the level of systemic inflammation.
- In untreated periodontitis, the same bacterial strains that are commonly found in periodontal pockets surrounding diseased teeth have been found in blood vessel plaques of those with CVD.
An indirect relationship has been shown between periodontitis and CVD, and many of the risk factors are shared in the two diseases. Cigarette smoking, especially, is common in determining the relative importance of risk in the relationship between the two. In addition to tobacco use, diabetes, obesity, systemic inflammation, high blood pressure, major depression, physical inactivity, family histories of CVD and periodontal disease, advancing age and male gender are other commonalities to both diseases.
We Shall Overcome — Treatment Based On The Evidence
And finally some great news! A great deal is known about the causes and successful treatment of inflammatory periodontal and cardiovascular diseases. While the mechanisms that link them are still the focus of ongoing research, their diagnosis and treatment individually and collectively can prolong your oral and general health. So, remember, united they stand, but divided they fall. Be sure to see your dental and medical health professionals to maintain your oral and general health and overall well-being.
Loose Dentures
Dear Doctor,
My dentures are so loose. I would like to have implants but I am unable to at this time. Can you please give me some information to help me better understand my options?

Dear Shanai,
It would seem from your question that you already understand that implants are your best option. What you may not be aware of is that over time, the continued compression of the tissues under full dentures results in loss of bone and gum tissue volume. The bone that formerly supported your teeth is not designed to withstand these forces, and in response, it resorbs or melts away over time resulting in what you are experiencing now, loose fitting dentures. The beauty of implants is that they stop the resorptive process by actually stabilizing the bone to prevent further loss.
Having said that, loose dentures are a common problem for people who are full or complete denture wearers, especially if you have worn them for a long time. Whether or not new dentures are needed depends not only upon the condition of your existing dentures, but also how much the supporting tissues have changed.
Over time, the continued compression of the tissues under full dentures results in loss of bone and gum tissue volume.
A number of questions therefore arise to determine the next best option to implants in an effort to stabilize your dentures:
- Are you satisfied with the appearance of your denture teeth?
- How worn are they?
- Is your bite still functional?
- Can you eat and chew properly?
Your dentist will help you assess if it is in your best interests to make new dentures or reline (refit) your existing dentures as an interim measure.
There are some tricks to improve the fit of your dentures temporarily. Relining dentures is generally necessary when full (removable) dentures become loose, after years of wear. Because the rate of bone loss differs from person to person, some denture wearers may need more frequent relines than others. Upper dentures tend to fit better and be less problematic than lower dentures because they have a much larger surface area on which to suction and rest.
There are two ways to reline your existing dentures:
- A temporary reline necessitates adding a layer of material under the denture in your mouth while you are in your dentist’s chair. This involves taking an impression (literally impressing material under the denture with a plastic or moldable material) that hardens and fills the void created where the oral tissues have shrunken away from the denture. This approach will generally stabilize the denture for a short period of time.
- A more permanent reline requires an indirect technique where material is added to the denture in the mouth in much the same way as described above for a temporary reline. However, the denture then needs to be sent to a dental laboratory to replace the temporary material with more permanent denture plastic, usually “methacrylate” (meth-a-cri-late). The advantage of a permanent reline is that it is longer lasting; although, it does mean that you will be without your denture for a day or more.
Dental implants are generally the best, if not only, option for long-term denture wearers with extremely loose fitting dentures.
If your dentist feels that a reline will not achieve the fit and stability desired, then remaking the dentures is the next option to consider. Other reasons for remaking the dentures are the wear of the denture teeth, poor esthetics, and poor condition of the denture’s base material.
In spite of the best efforts of the dentist and laboratory, satisfaction cannot be guaranteed with the fit and function of previously loose dentures, particularly if you have extensive bone and gum tissue loss. At this stage it may be best to consider any reline option temporary. This is the reason why dental implants are generally the best, if not only, option for long-term denture wearers with extremely loose fitting dentures.
A new denture, particularly a lower one, can be successfully supported by implants. There are a number of options including mini-implants or as few as two implants (the minimum) that can provide stability for a denture. And because you will not need every tooth replaced by an implant, the cost is not as great as you may think. In fact, many people find implants to be a feasible and realistic solution once they compare the ongoing maintenance and discomfort of ill-fitting dentures to the cost and benefit implants provide with many years of successful and stable denture wear.
Improved function, biting, chewing, talking, and smiling will provide you with improved self-confidence and well-being with relined, renewed dentures or implant supported dentures. Ask your dentist about financing plans or consider saving over time so that dental implants can ultimately help resolve your denture problem in a more long-term way.
Standard of Care for Edentulous Patient
A New Standard of Care — Two Implants will change Everything!
The two-implant overdenture for the lower jaw is a far simpler and equally effective solution. In fact, in the original Toronto Study (when the treatment was introduced to North America), the complaints of many patients seeking implant treatment were solved during the initial healing phase as their lower denture — fitted or relined over the implants — provided them with an increase in retention, stability and comfort.
| A Closer Look at the Implant Overdenture |
| The lower jaw “overdenture” fits securely onto the two dental implants and is removable by the individual for cleaning purposes and may or may not be left out at night. |
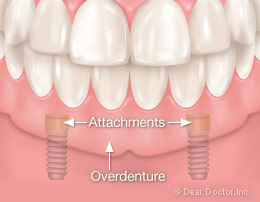 |
| Illustration showing an example of two implants for attachment and stabilization of the mandibular denture. |
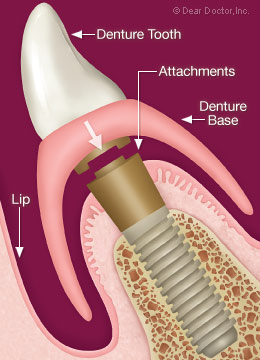 |
| A cross-section illustration showing how the denture attaches to the implants. |
Studies over the past decade have continued to demonstrate the enormous benefits of lower jaw overdenture treatment. Results have led to the development of what is called the McGill Consensus Statement on Overdentures (May 2002) which states “As a minimal treatment objective: the mandibular (lower jaw) two-implant overdenture (as opposed to a conventional denture) should be considered as a first choice standard of care for the edentulous patient.”
What is the science supporting this new minimal treatment objective? When one examines the impact of this treatment on edentulism, the results can only be defined as remarkable! Perhaps the most important consideration is that implants will significantly reduce the destructive resorptive bone-loss process — by about 75 percent less in the areas the implants are placed as compared to the use of dentures without implant treatment.
Since the preservation of remaining bone structure is a major cornerstone of modern dentistry, the prevention of further bone loss is a key element in the success of overdenture treatment. Also, since most of the bone loss occurs within the first year after tooth loss, it is most ideal if implants are placed during the first year after tooth loss rather than waiting until later. Thus, the utilization of implants to preserve bone is in and of itself a sufficient rationale to recommend this treatment.
While implant overdentures improve mastication (chewing), does this result in improved nutrition? When comparing the lower two-implant overdenture to conventional dentures researchers determined that altered eating habits are reflected in a comparison of blood parameters. They showed that there were significant increases in concentrations of serum albumen, hemoglobin, B12 and carotene in the lower two-implant overdenture group and no changes in the conventional denture patients. This and other clinical data suggest that providing edentulous patients with one of the least complicated forms of implant dentistry gives patients the opportunity to modify their diets and improve nutrition, which may impact their general health.
Additionally, other evidence suggests that quality of life ratings for oral health are higher for individuals who receive two-implant overdentures than for those with new conventional dentures. No more loose dentures or embarrassing moments in public trying to eat or speak. Patients report an improved self-perception of facial attractiveness. This is of considerable importance, indicating that this simple implant rehabilitation may actually restore a patient’s quality of life.
So, you may be asking am I a candidate for this treatment? Generally, if a person is healthy enough to undergo a tooth extraction, then they are also a candidate for the two-implant overdenture treatment. The entire surgical phase can often be completed in one visit, although careful assessment and pre-planning are necessary pre-requisites.
Potential candidates include the dissatisfied denture patient suffering from discomfort and lack of retention of their lower denture, as well as partially edentulous patients with severely compromised teeth that cannot successfully support a prosthesis whether fixed or removable. Research has shown that neither increasing age nor osteoporosis is a barrier to successful healing or integration of implants.
Can this simple treatment be applied to my upper denture? NOT EXACTLY. Upper implant overdentures have different needs and requirements for success and predictability when compared to the lower implant overdenture. Based on differences in bone volume, density and other anatomic factors, preliminary evidence suggests that at least four, and in some cases as many as six implants are needed to retain an upper (maxillary) implant overdenture. The upper two-implant overdenture should not be considered a standard procedure at this time — more research is needed. So, the case selection is different and more difficult for the upper jaw — it is more costly and comparatively more complex. Please consult your dentist if you are considering an upper implant overdenture.
In Conclusion
The lower two-implant overdenture represents a simple, effective and predictable solution to the problem of edentulism. Since the treatment only requires two implants for most people to restore an entire jaw, it is within the financial reach of many so afflicted people. It results in a remarkable improvement in oral comfort and a significantly improved ability to chew most foods, and consequently a person’s nutritional status. It eliminates expensive denture creams and adhesives along with their potential medical side effects.
Most importantly, studies indicate a consistently high level of patient satisfaction for the two-implant overdenture when compared to the conventional denture, and a general improvement in quality of life. This represents a major change for the dental profession and the public in the management of edentulous patients, suggesting that the lower two-implant overdenture may be considered the more appropriate starting point over regular dentures. If your dentist does not recommend this treatment for you, then you may want to ask about it. This simple treatment can profoundly change someone’s life for the better — maybe yours or someone you know!
Additional Questions About Lower Implant Overdentures
- My dentist wants to retain and repair a few teeth and fabricate a new partial denture — does that make sense?This depends on the number, position, decay rate, periodontal status and the costs needed to retain the remaining teeth. Evaluating the amount of remaining bone in the front part of the jaw (ideally requiring CT scans) is also used to consider whether or not removing questionable teeth and fabricating an overdenture will provide you with a more long-term predictable outcome.
- Will it be painful?Studies indicate that following dental implant placement most patients will experience only minor discomfort on the first day, with a rapid improvement by the second day, often with less pain as compared to an extraction (tooth removal) procedure.
- Will I need a new denture?One method to further reduce cost is to explore whether or not one’s existing denture can be converted to an implant overdenture — this needs to be evaluated by a dentist based on a number of factors and can be determined before the start of treatment.
- Is it expensive?Although the total cost may be several times that of a conventional denture, it is a much less expensive than restoring an entire jaw with implants, and is a fraction of the costs of fixed implant bridges. Cost for most patients should not be a barrier to gain the benefits of this treatment, especially if one considers the years of service implant overdentures would provide and the money saved with the continued use of dental adhesives.
- How long will it take to complete?From start to finish, all phases of treatment can be completed in about three to four months and the fabrication of the implant teeth can be completed without any local anesthetic.
- My dentist recommended four implants to fabricate a lower implant overdenture — Is that advisable?While long term studies clearly indicate that two implants are sufficient to predictably retain a lower overdenture for most people, there are some advantages additional implants can provide. Please consult with your dentist so that he can discuss your specific needs.
Dentists Diagnose Diabetes
Dental visits can aid in the process of diagnosing diabetes or prediabetes for people with the condition, according to researchers at the Columbia University College of Dental Medicine.
The reason for this possibility is that when a patient has periodontal disease, that’s one of the first complications associated with diabetes.
Dentists haven’t played a role in identifying diabetes in the past, so this may be a vital step toward curbing the problem.
To compile the data, researchers recruited about 600 people who visited a dental clinic in Manhattan. The people had to be at least 40 or the person had be 30 or older of if he she was Hispanic or nonwhite. These people also had never been told they had diabetes.
Around 530 of the people with at least one diabetes risk received a periodontal examination and a finger stick to test hemoglobin. The patients then came back for a plasma glucose test to determine if the person has diabetes or a prediabetes condition.
Based on their findings, researchers could make the correlation that for the at-risk dental population, one algorithm—based on the number of missing teeth and a plethora of deep periodontal pockets—could proficiently recognize patients with diabetes or prediabetes that hadn’t been recognized before. To double check this information, researchers used a point-of-care hemoglobin A1c test.
If dentists and periodontists pay attention to these periodontal issues, it will be pivotal in diagnosing diabetes earlier than it has been in the past.
How Crowns Attach to Dental Implants
Dear Doctor,
I was intrigued to learn that implant crowns can either be screwed into implants or cemented on to them. Wouldn’t a screwed-in crown look awful? Why would I want to have my crown attached this way?
 |
| Once a crown is attached to the implant, a person cannot determine which method of attachment was used (from the frontal view). |
Dear Jake,
I can understand your concerns; after all, you want your replacement tooth to function well, and look perfectly natural. Rest assured, you can have both with either a “screwed-in” or “cemented” implant crown.
While implants replace teeth, they are artificial and behave differently from natural teeth. A quick recap will be helpful in explaining why. A dental implant is a tooth-root replacement, to which an implant crown is attached. The crown is the only part you see in the mouth. The implant is placed surgically in the bone of the jaw to which it fuses in a process called osseo-integration (“osseo” – bone; “integrate” – to join or fuse). A great deal of thought, research and ingenuity has gone into dental implant tooth-replacement systems to make them as fail-safe as possible. Over and above what you see, there are many other clinical aspects and considerations involved in their design and functionality to protect and maintain implant survival.
 |
| Cemented Crown vs. Screw-Retained Crown Click to enlarge |
Dental Implants — Dental Legos
Screws facilitate the attachment of the implant crowns to the implants. Implants must be strategically placed to allow implant crowns to connect to them, so that the crowns emerge through the gum tissues in exactly the right direction. An adjoining support structure called an “abutment” is often used to allow for this transition and connection.
Like Legos, implant components are designed to disassemble. Screw-retained implant crowns are more easily maintained; they allow forretention — keeping abutments and implant crowns in place, and retrievability — allowing the implant-crown components to be more easily removed, repaired or replaced, without damaging the implant or the restoration. While a successful dental implant can last a lifetime, most crowns do not. They may need to be replaced or repaired periodically, and this is much easier to do if they are attached with screws.
Loosening of the screw that attaches the restoration to the implant occasionally happens. Retightening or replacing the screw when the restoration is screw-retained is a simple and predictable procedure. This cannot be said for cemented restorations. Cemented crowns can be difficult to remove and, in the worst case, a screw access hole may have to be put in to remove the abutment and crown from the implant. Creating a screw access hole in the back teeth is not a cosmetic problem but for the front teeth, creating the screw access hole may affect the crown’s appearance. It is difficult to know where the screw exit is located and often crowns removed in this fashion have to be remade. A weaker cement can be used to facilitate removal but this can lead to an insecurely attached crown falling off the abutment during use.
Aesthetic Considerations

People can object to screw-retained crowns believing that they may be unsightly — and in places, that might be true. That’s why implant crowns are cemented to abutments whenever screws would show. Cemented restorations can accommodate more implant positions by covering abutment screw holes completely.
Screw-retained restorations can only be used in areas where the screw access holes are not so conspicuous, like the biting surfaces of back teeth. These access holes can be filled with composite tooth-colored filling material, rendering them essentially invisible to all but the dentist.
Keep in mind that cementation, too, can be problematic: Removal of excess cement, particularly if the implant-to-crown connection is deep within the tissues, can be difficult.
Screws Are Safer In Certain Situations
Immediately Loaded Implants
Screw-retained crowns are easier to manage when implants are crowned immediately. An implant is usually left in place for several months to fuse to the bone (osseo-integrate) before a crown is attached. But in some cases, the crown will be attached at the same time that the implant is placed — a process referred to as “immediate loading.” Here, screws offer additional advantages over cement. Sometimes the cement seal can be lost during the critical six-to-eight-week initial healing period or the cement can cause inflammation if it flows below the gum tissues.
Provisional Implant Crowns
To develop ideal aesthetics, a provisional (customized temporary) crown is required to shape and mold the soft gum tissues. The simplest method is to use a screw-retained provisional restoration. The screw can actually be used to “seat” the provisional crown and gently expand and accommodate the gum tissues.
Long-Term Treatment Planning
This topic is an extension of retrievability. Given the long-term survival characteristics of today’s dental implants, they can outlast neighboring natural teeth that ultimately succumb to decay or periodontal disease. In these situations, the implants can often be used to support bridges if more natural teeth are lost. Sometimes even the substructures (the implants and abutments) of the existing implant crowns can be incorporated into the new bridgework. Screws play an important role in being able to retrieve and re-use existing implant restorations.
So as you can see, screwed-in crowns and cements have advantages and disadvantages. Your dentist will recommend which option is best for you.
Call Roslyn Office Phone Number (516) 484-6394 to schedule an appointment with Dr. Gardner.
Complete our .
Mouthguards and Sports
Many children that don’t wear protective mouthguards while playing sports should be doing so, according to a survey conducted by Delta Dental Plans Association. These findings indicate that children aren’t listening to their dentists.
Delta Dental recently did a wide-ranging survey regarding the oral health of American children.
Aside from the obvious protection provided to the teeth, mouthguards absorb shock and soften a blow that could have resulted in a concussion. The US Centers for Disease Control and Prevention calculated that around 300,000 people suffer sports-related concussions every year—children and teenagers are at the highest risk.
About seven of 10 parents reported that their child doesn’t wear a mouthguard for sports like baseball, basketball, soccer or softball. Parents of athletes in these sports are less fearful of injury than if their child played hockey, lacrosse or football, for example. Studies, however, indicate that basketball players are 15 times more likely to experience an orofacial injury than a football player is.
Since mouthguards became mandatory for football players, mouth injuries have declined significantly. Still, only about 70 percent of parents claimed their child always wears a mouthguard during practices and games. Around 44 percent of hockey parents said their child wore a mouthguard for games and practices.
The three kinds of mouthguards available include: (1) stock mouthguards, which are the least expensive; (2) mouth-formed mouthguards, which can be purchased at sporting goods stores and can conform to the child’s mouth; and (3) custom-made mouthguards, the most expensive choice, which are made from a dentist and are molded to the child’s teeth.
Regardless of how much money a parent wants to pour into mouth protection, any mouthguard is better than nothing.
Immediate Loading of Dental Implants
What was nearly impossible just a short time ago, Dr. Gardner now makes happen hundreds of times each year! You can receive beautiful new teeth, in just one day!
Advances in implant technology and new protocols developed by experienced Doctors allow for less invasive surgery without bone grafts that results in the ability to replace failing or missing teeth with customized, hand-crafted replacements immediately or soon thereafter.
This can be done with ONE tooth or MULTIPLE teeth and eliminates the need for a removable temporary appliance while maintaining near normal function during the healing phase. Since the teeth are fixed to implants, there is usually a shorter adjustment period.
Not everyone is a candidate for this procedure. A clinical exam is necessary to determine the right conditions. Teeth delivered at the time of surgery are provisional (temporary) teeth, and will be changed to a final prosthesis after complete healing. The provisional teeth can be used for as long as a year. This process is called Immediate Loading and is carried out in a predictable fashion as long as patients meet the necessary criteria. Immediate Loading is a procedure I enjoy most and consider it to be one of the many modern miracles in Dentistry.